Introduction
Bronchiectasis is a chronic and heterogeneous respiratory disease characterized by abnormal and permanent dilation of the bronchi, chronic cough, sputum production, recurrent respiratory infections, and progressive airflow limitation. Historically considered a localized airway disorder, bronchiectasis is now widely recognized as a systemic disease with important extrapulmonary manifestations that significantly influence functional status, quality of life, and prognosis. Among these systemic consequences, skeletal muscle dysfunction has gained increasing attention as a major determinant of exercise limitation and disability.
Skeletal muscle dysfunction in bronchiectasis encompasses a range of abnormalities, including reduced muscle strength, impaired endurance, decreased oxidative capacity, and alterations in muscle mass and composition. These changes may be present even in patients with mild-to-moderate pulmonary impairment, suggesting that factors beyond lung mechanics contribute to muscle involvement. Sarcopenia, defined as the combined loss of muscle mass and muscle function, represents a more advanced and clinically impactful manifestation of muscle impairment.
Recent studies, including those published by our group,1,2 have provided contemporary evidence demonstrating that muscle dysfunction and sarcopenia are prevalent in chronic respiratory diseases such as bronchiectasis and are associated with disease severity, reduced exercise capacity, and poorer functional outcomes. These findings reinforce the concept of bronchiectasis as a systemic disease and highlight the need to better understand the mechanisms underlying skeletal muscle impairment. This review aims to summarize current clinical evidence and discuss the most relevant biological mechanisms involved in skeletal muscle dysfunction and sarcopenia in bronchiectasis. This review further outlines potential therapeutic strategies to combat sarcopenia in patients with bronchiectasis.
Muscle dysfunction and sarcopenia in bronchiectasis
Sarcopenia is closely linked to muscle dysfunction in patients with bronchiectasis, manifesting as reduced muscle mass, strength, and endurance, which negatively impact clinical outcomes. In bronchiectasis, impaired muscle function – particularly reduced leg strength and core endurance – has been shown to correlate with worse dyspnea, decreased health-related quality of life, and diminished functional capacity over time.3–5 This relationship is underpinned by altered body composition, including lower appendicular muscle index and increased prevalence of osteopenia, especially in females with bronchiectasis.3
The pathophysiology involves systemic factors such as chronic inflammation, physical inactivity, and nutritional deficits, which drive muscle catabolism and atrophy, leading to sarcopenia and subsequent muscle dysfunction.5 Sarcopenia in chronic respiratory diseases is also associated with reduced respiratory muscle strength and function, further contributing to exercise intolerance and disability.2,6 The Japanese Association of Rehabilitation Nutrition defines respiratory sarcopenia as the coexistence of whole-body sarcopenia and low respiratory muscle mass and strength, which can progress to sarcopenic respiratory disability if functional impairment develops.6 Sarcopenia and muscle dysfunction are interrelated in bronchiectasis, with sarcopenia contributing to impaired muscle function and both conditions jointly worsening clinical outcomes such as dyspnea, quality of life, and exercise capacity.3–6
Clinical studies consistently report the presence of peripheral skeletal muscle dysfunction in patients with bronchiectasis. Reduced muscle strength, particularly in the lower limbs, is one of the most frequently described abnormalities and can be detected using simple clinical tools such as quadriceps or handgrip strength assessment. Importantly, muscle weakness has been reported even in patients with preserved lung function, indicating that skeletal muscle impairment cannot be fully explained by airflow limitation alone.
In recent studies published by our group,2 we demonstrated that patients with bronchiectasis exhibit significant reductions in lower-limb muscle strength compared with reference values. Muscle strength was strongly associated with exercise performance, while its relationship with pulmonary function was weaker, supporting an independent contribution of peripheral muscle dysfunction to exercise limitation. Furthermore, ultrasonography revealed decreased muscle thickness and area, whereas magnetic resonance imaging demonstrated increased fat infiltration, which positively correlated with the bronchiectasis severity scores.2 Structural parameters (proportions of hybrid fibers, internal nuclei, abnormal fibers, and apoptotic nuclei) were significantly greater in the vastus lateralis of patients than in controls and inversely correlated with quadriceps muscle function and exercise capacity in the former.2
Beyond strength deficits, patients with bronchiectasis frequently exhibit reduced muscle endurance and impaired aerobic capacity. These abnormalities contribute to early muscle fatigue during exercise and daily activities.4–6 Reduced physical activity levels are commonly observed and are closely linked to muscle dysfunction, creating a vicious cycle of inactivity, deconditioning, and further functional decline.4–6 Skeletal muscle dysfunction has important clinical consequences, including reduced exercise tolerance, increased dyspnea and fatigue, impaired quality of life, and reduced ability to cope with disease exacerbations. Collectively, these findings highlight skeletal muscle impairment as a key extrapulmonary feature of bronchiectasis with major functional relevance.2–6
Mechanisms leading to muscle dysfunction and sarcopenia in bronchiectasis
Clinical factors
The clinical factors that lead to muscle dysfunction and sarcopenia in patients with bronchiectasis include older age, female sex, lower body mass index (BMI), increased dyspnea, reduced exercise capacity, and frequent exacerbations.2–6 These factors are associated with reduced peripheral muscle strength, impaired core endurance, and altered body composition, such as decreased appendicular muscle index and increased prevalence of osteopenia, particularly in females (Fig. 1).3–6
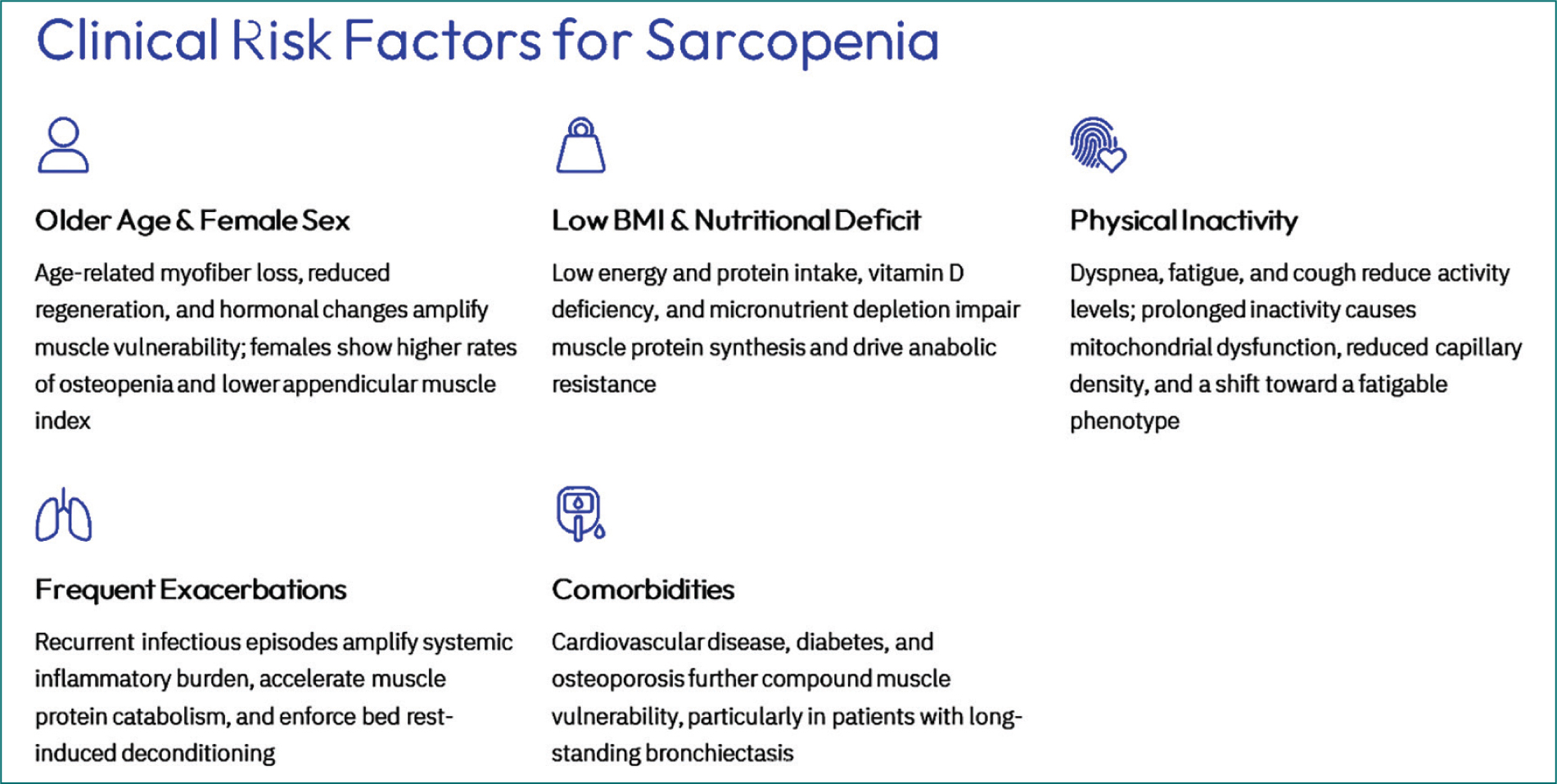
Figure 1. An overview of the most relevant clinical contributors to sarcopenia and muscle dysfunction in patients with bronchiectasis.
Physical inactivity and deconditioning represent major contributors to muscle dysfunction. Symptoms such as dyspnea, fatigue, and cough often lead patients to reduce their physical activity levels. Prolonged inactivity results in reduced oxidative enzyme activity, mitochondrial dysfunction, decreased capillary density, and a shift toward a more fatigable muscle phenotype. Physical inactivity also interacts with inflammation and aging, amplifying muscle impairment.
Aging and comorbidities such as cardiovascular disease, diabetes, and osteoporosis further increase vulnerability to muscle dysfunction, particularly in patients with long-standing disease (Fig. 1).3–6
Biological mechanisms
The mechanisms underlying skeletal muscle dysfunction in bronchiectasis are complex and multifactorial, involving the interaction of disease-related, behavioral, and host-related factors. Chronic systemic inflammation plays a central role. Persistent airway infection and inflammation can lead to the release of pro-inflammatory mediators into the systemic circulation, promoting catabolic signaling pathways in skeletal muscle and impairing protein synthesis. Recurrent exacerbations may further amplify this inflammatory burden and accelerate muscle decline. Studies investigating the mechanisms involved in the pathophysiology of sarcopenia in patients with bronchiectasis are currently underway. However, based on the existing literature in patients with chronic obstructive pulmonary disease (COPD), it is reasonable to assume that several of the underlying mechanisms may also be shared with bronchiectasis-associated sarcopenia.
Chronic systemic inflammation, recurrent infections, oxidative stress, physical inactivity, nutritional deficits, and hormonal imbalances drive muscle dysfunction and sarcopenia in bronchiectasis.7–9 Neutrophil-driven airway inflammation, elevated neutrophil elastase, and cytokine release contribute to muscle catabolism and impaired regeneration, as previously shown in the limb muscles of patients with COPD.10–15 Oxidative stress and mitochondrial dysfunction further promote muscle wasting and reduce muscle function in patients with other chronic respiratory diseases, namely COPD.11,12,16–22 Age-related changes, including reduced myofiber size and number, increased fat infiltration (myosteatosis), and altered muscle-bone endocrine signaling, exacerbate sarcopenia in bronchiectasis.2,10 In addition, impaired mucociliary clearance and hypoxia may indirectly worsen muscle dysfunction by increasing disease severity and limiting physical activity in these patients.9
Alterations in muscle protein metabolism are another key mechanism. An imbalance between protein synthesis and degradation favors muscle wasting, driven by increased activation of proteolytic pathways and reduced anabolic signaling in COPD-associated sarcopenia.11,13,16 Anabolic resistance, particularly in older patients, may also limit the muscle response to nutritional intake and exercise. Exposure to systemic corticosteroids, when present, may exacerbate muscle protein breakdown in both COPD and bronchiectasis patients with sarcopenia.
Hypoxemia and oxidative stress further contribute to skeletal muscle dysfunction. Chronic or exertional hypoxemia impairs mitochondrial oxidative phosphorylation, whereas increased reactive oxygen species (ROS) production leads to oxidative damage of muscle proteins and organelles. Nutritional abnormalities, including low energy intake, protein deficiency, and micronutrient deficits, are common in bronchiectasis patients and contribute to their reduced muscle mass and function.9,11–13,16
Oxidative stress in blood and muscles, as well as endoplasmic reticulum (ER) stress, are central contributors to the development of muscle dysfunction and sarcopenia in patients with COPD and bronchiectasis. In bronchiectasis, systemic and muscle-specific oxidative stress is characterized by elevated levels of ROS, increased protein carbonylation, and reduced antioxidant defenses such as catalase and superoxide dismutase activity. This redox imbalance directly impairs muscle contractility, promotes protein degradation via activation of proteolytic pathways (e.g., ubiquitin-proteasome system), and disrupts mitochondrial function, leading to muscle atrophy and reduced physical capacity11–20,23,34 in patients with COPD and bronchiectasis. ROS also activates redox-sensitive signaling pathways (NF-κB, FoxO), which further drive muscle catabolism and structural disruption (Fig. 2).11,34
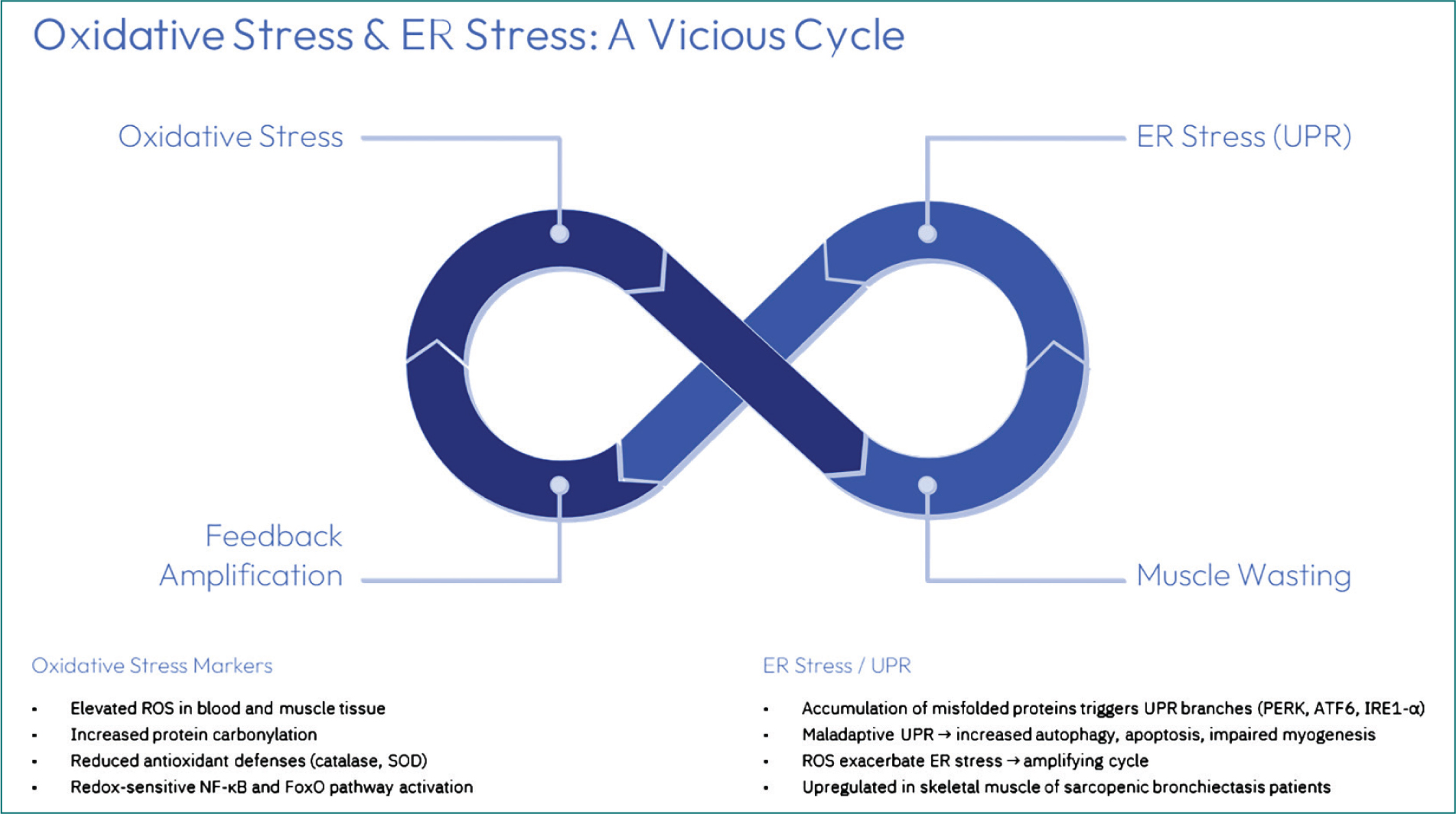
Figure 2. An overview of the interrelation between biological mechanisms such as oxidative stress and endoplasmic reticulum (ER) stress in skeletal muscles of patients with bronchiectasis.
ER stress arises when misfolded or unfolded proteins accumulate in the ER, triggering the unfolded protein response (UPR). In respiratory diseases, including bronchiectasis, ER stress is upregulated in skeletal muscle, particularly in sarcopenic patients. This maladaptive response activates UPR branches (PERK, ATF6, IRE1-α), leading to increased autophagy, apoptosis, and impaired muscle regeneration, which contribute to muscle wasting and weakness in patients with COPD.35,36 ROS generated during oxidative stress may also exacerbate ER stress, creating a vicious cycle that amplifies muscle dysfunction in COPD.35–37 In patients with bronchiectasis, ER stress was also shown in the quadriceps muscle (unpublished observations).
Together, oxidative stress and ER stress synergistically promote muscle protein degradation, impair muscle repair, and accelerate sarcopenia in bronchiectasis, resulting in reduced muscle mass, strength, and functional capacity (Fig. 2).11,25,27,28,33–38
Muscle dysfunction and sarcopenia in bronchiectasis arise from a combination of clinical risk factors and biological mechanisms, including chronic inflammation, oxidative stress, physical inactivity, nutritional deficits, and hormonal changes, all of which contribute to reduced muscle mass, strength, and function.11,25,27,28,33–38
Sarcopenia as a multidimensional clinical entity in bronchiectasis
Sarcopenia represents a clinically meaningful manifestation of skeletal muscle impairment in bronchiectasis. Using contemporary diagnostic criteria, recent studies2–6 have reported a high prevalence of sarcopenia in patients with bronchiectasis. Sarcopenia is associated with reduced muscle strength, impaired physical performance, and greater disease severity.
Importantly, these studies demonstrated that sarcopenia in bronchiectasis is not solely driven by low body weight or reduced lung function, but rather reflects a multidimensional process involving muscle mass, muscle quality, and physical performance. Sarcopenia was associated with worse functional outcomes and greater systemic disease burden, supporting its relevance as a clinical marker and therapeutic target.2,4–6,24
Despite its clinical importance, sarcopenia remains underrecognized in routine practice. Integrating muscle mass and strength assessment into the evaluation of patients with bronchiectasis may allow earlier identification of high-risk individuals and more personalized management strategies.
Therapeutic interventions
Exercise training is a cornerstone intervention for skeletal muscle dysfunction and sarcopenia in bronchiectasis. Resistance training is particularly effective in improving muscle strength and mass, while endurance training enhances oxidative capacity and fatigue resistance. Pulmonary rehabilitation programs tailored to patients with bronchiectasis have demonstrated improvements in exercise tolerance, physical activity levels, and quality of life.39–45
Nutritional optimization is essential to support muscle maintenance and adaptation to exercise. Adequate energy and protein intake should be ensured, and nutritional supplementation may be beneficial in selected sarcopenic patients. Addressing vitamin D and other micronutrient deficiencies may provide additional benefits.40–44,46–49 Disease-targeted strategies aimed at reducing airway infection, controlling inflammation, and preventing exacerbations may also indirectly benefit skeletal muscle by reducing systemic inflammatory burden and metabolic stress. Given the multifactorial nature of muscle dysfunction, integrated multidisciplinary approaches are likely required (Fig. 3).41,44,45,49–51
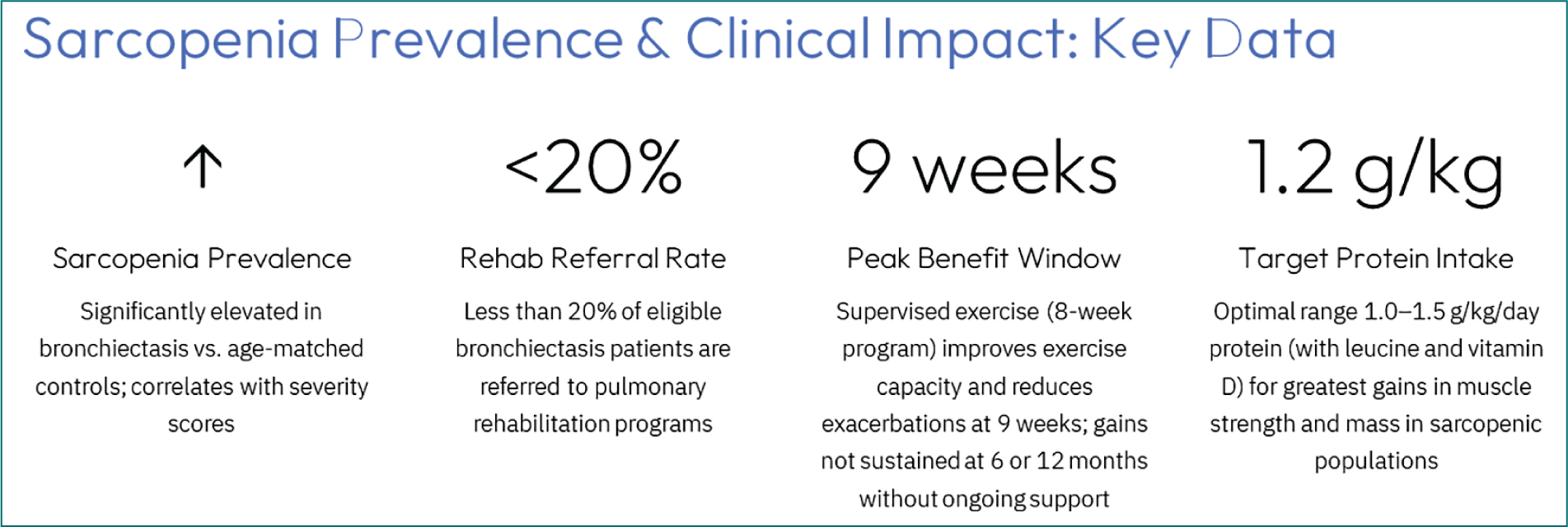
Figure 3. An overview of the clinical impact of sarcopenia in patients with bronchiectasis and therapeutic options. Structural muscle abnormalities (hybrid fibers, internal nuclei, apoptotic nuclei) in the vastus lateralis inversely correlate with quadriceps function and exercies capacity (Alvarado-Miranda et al.).2
The most effective evidence-based interventions to prevent or reverse muscle dysfunction and sarcopenia in patients with bronchiectasis are structured exercise training (especially resistance and balance training), optimized protein-based nutritional support, and pulmonary rehabilitation.40–51
Supervised exercise training, including resistance and aerobic modalities, improves functional exercise tolerance, muscle strength, and quality of life in bronchiectasis, with clinically meaningful gains in walk distance and reduced exacerbation rates immediately post-intervention. However, sustained benefits require ongoing participation, as effects diminish after cessation of structured programs.39,44,48,49 Pulmonary rehabilitation is specifically recommended for bronchiectasis patients with impaired exercise tolerance by the European Respiratory Society and the British Thoracic Society (Fig. 3).39,44,51
Combining resistance and balance training with protein-based nutritional supplementation (e.g., 1.0-1.5 g/kg/day protein, with leucine and vitamin D) yields the greatest improvements in muscle strength, mass, and physical function in general sarcopenic populations, and this approach is supported by high-certainty evidence.42,44,46,47 Adequate protein intake, anti-inflammatory nutrients (such as omega-3 fatty acids), and probiotics may further enhance muscle health and reduce inflammation, which is relevant given the chronic inflammatory milieu in bronchiectasis.39,46
Anti-inflammatory pharmacologic therapies (e.g., corticosteroids) are not routinely recommended for bronchiectasis unless there is coexisting asthma or COPD, due to infection risk.9,50 Instead, non-pharmacologic anti-inflammatory strategies – such as exercise and nutrition – are prioritized. The optimal approach is a multimodal intervention combining resistance and balance exercise, protein-rich nutrition, and pulmonary rehabilitation, tailored to the patient’s functional status and comorbidities (Fig. 4).42,44,46–49
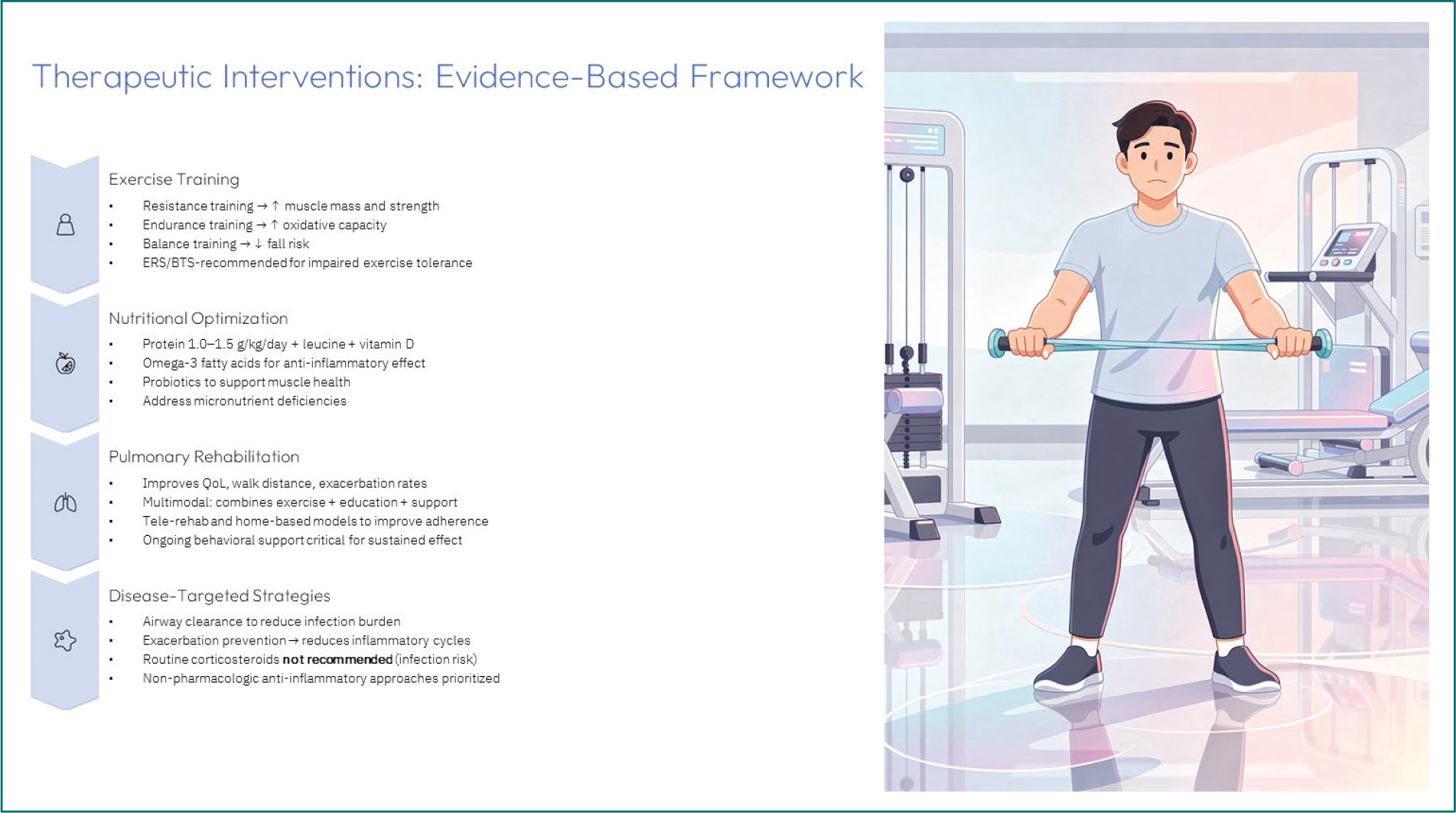
Figure 4. A general overview of the different therapeutic interventions in patients with bronchiectasis.
In patients with bronchiectasis, the latest randomized controlled trials and meta-analyses show that multimodal interventions – specifically resistance and balance exercise combined with protein-rich nutrition and pulmonary rehabilitation – produce clinically meaningful short-term improvements in muscle strength, mass, and physical function in patients with sarcopenia, including those with chronic respiratory diseases such as bronchiectasis. However, long-term sustainability and adherence rates are suboptimal, with benefits often diminishing after cessation of structured programs.5,42,51–54 It should be mentioned that in meta-analyses and systematic reviews of interventions in general sarcopenia and in bronchiectasis patients, the populations were predominantly older adults (median age > 70 years), with a high proportion of women, and included both community-dwelling and institutionalized individuals, but studies specific to bronchiectasis focused on ambulatory, non-institutionalized adults with stable disease.42,53,55 Randomized controlled trials and longitudinal studies enrolled adults with established bronchiectasis, frequently excluding those with cystic fibrosis, significant comorbidities, or severe malnutrition, with limited generalizability (Fig. 4).42,53,55
In bronchiectasis patients, a randomized control trial with 12-month follow-up demonstrated that supervised exercise training (8 weeks) followed by monthly telephone support improved exercise capacity and reduced exacerbations at 9 weeks, but these gains were not sustained at 6 or 12 months, highlighting challenges in long-term adherence and maintenance of effect.39,51 Meta-analyses in sarcopenia populations confirm that resistance and balance training with protein supplementation yields the greatest improvements in grip strength, gait speed, and muscle mass, but most trials have intervention durations of 8-24 weeks, and sustained effects beyond this period are rarely observed unless ongoing support or structured follow-up is provided (Fig. 4).42,53,55,56
Adherence rates to pulmonary rehabilitation and exercise programs in bronchiectasis patients are low, with < 20% of eligible patients referred and even fewer completing long-term programs.51 Strategies to improve sustainability include ongoing behavioral support, integration of home-based or tele-rehabilitation models, and individualized, progressive exercise prescriptions (Figs. 3 and 4).40,51,57
Multimodal interventions are effective in the short term, but long-term sustainability and adherence remain major challenges, with benefits waning after program completion unless ongoing support is provided.
Despite growing recognition of skeletal muscle dysfunction and sarcopenia in bronchiectasis, important research gaps remain. Much of the current knowledge is derived from cross-sectional studies or extrapolated from COPD, while disease-specific mechanistic investigations in bronchiectasis are still limited. The relative contribution of biological processes such as systemic inflammation, oxidative stress, mitochondrial dysfunction, and altered muscle protein metabolism requires further clarification. In addition, standardized approaches for the identification and monitoring of sarcopenia in bronchiectasis are lacking. Future longitudinal studies and well-designed randomized trials are needed to better define the natural history of muscle impairment and to evaluate targeted multimodal interventions in this population.
Conclusion
Skeletal muscle dysfunction and sarcopenia are important and underrecognized extrapulmonary manifestations of bronchiectasis. Sarcopenia and muscle dysfunction in patients with bronchiectasis are driven by a multifactorial interplay of clinical and biological factors, including older age, female sex, low BMI, physical inactivity, frequent exacerbations, and chronic inflammation.58,59 Oxidative stress in blood and muscle tissue, as well as ER stress, further contribute to muscle catabolism, impaired regeneration, and mitochondrial dysfunction, exacerbating muscle loss and weakness (Fig. 5).40,41,60
Figure 5. Schematic representation of the key concepts discussed in the review.
Evidence-based interventions focus on resistance and balance training, pulmonary rehabilitation, and protein-rich nutritional support, which together improve muscle strength, mass, and functional outcomes; however, long-term sustainability and adherence are limited without ongoing behavioral or technological support.10,61,62 Patient populations in relevant studies are typically adults with non-cystic fibrosis bronchiectasis, characterized by impaired exercise tolerance, reduced muscle strength, and a range of nutritional and functional statuses, with most studies excluding those with severe comorbidities or recent exacerbations (Fig. 5).59
Overall, an integrated, multimodal approach is required to address sarcopenia and muscle dysfunction in bronchiectasis, targeting both clinical and molecular mechanisms while recognizing the challenges of maintaining intervention effects over time. Early recognition and targeted, multidisciplinary interventions addressing both pulmonary and systemic factors are essential to improve functional status and prognosis in patients with bronchiectasis.
Funding
The research conducted in our group has been supported by SEPAR-2020, PI21/00215 and PI24/00204 (Funded by ISC-III and co-funded by the European Union), BA21/00003, Intensificaciones INT19/00002 and INT22/00008, 2021-SGR-00100, CIBERES (ISC-III), Laboratorios Menarini Spain, SLT028/23/000016.
Conflicts of interest
None.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from all patients, and secured approval from the Ethics Committee. SAGER guidelines have been followed as applicable to the nature of the study.
Declaration on the use of artificial intelligence. The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
