Introduction
Chronic obstructive pulmonary disease (COPD) is the third leading cause of mortality and a top-10 cause of disability worldwide.1 COPD is characterized by airflow limitation, resulting from airway inflammation and remodeling, together with destruction of lung parenchyma.2 Beyond respiratory impairments, approximately 50% of patients with severe COPD develop muscle dysfunction,3 primarily affecting the lower limbs.4 The quadriceps femoris muscle, in particular, exhibits profound structural and metabolic alterations, including reduced mitochondrial density and diminished activity of the Krebs cycle enzymes.5 In addition, patients with COPD exhibit a shift toward a more glycolytic fiber-type profile, with a lower proportion of type I oxidative fibers,6 decreased capillarization,7 and reduced muscle fiber cross-sectional area.6 Collectively, these alterations contribute to the decline in muscle strength and endurance, ultimately impairing functional performance, including locomotion, activities of daily living, and quality of life.8,9
Skeletal muscle (SkM) dysfunction in COPD reflects the interaction of multiple pathophysiological alterations, including systemic inflammation, oxidative stress, and hypoxia.10,11 In parallel, several clinical factors such as physical inactivity, exacerbation burden, corticosteroid exposure, and nutritional status may further aggravate the muscle phenotype and contribute to functional decline.12 However, whether muscle dysfunction arises primarily from the pulmonary disease itself or is secondary to physical inactivity remains a matter of ongoing research.13 Increasing evidence suggests that disease-related systemic factors and physical inactivity interact bidirectionally, forming a self-perpetuating cycle in which pulmonary and systemic abnormalities promote physical inactivity, which in turn accelerates muscle deconditioning and metabolic dysfunction.14,15 Notably, SkM impairment is a common early clinical manifestation in patients with COPD. It can be detected even in those with mild-to-moderate airflow obstruction (Fig. 1A).16,17 Importantly, muscle dysfunction has also been linked to adverse clinical outcomes, including poorer survival,18,19 increased hospital readmission, greater need for mechanical ventilatory support (i.e., increased health care resource utilization), and higher morbidity and mortality.2,20
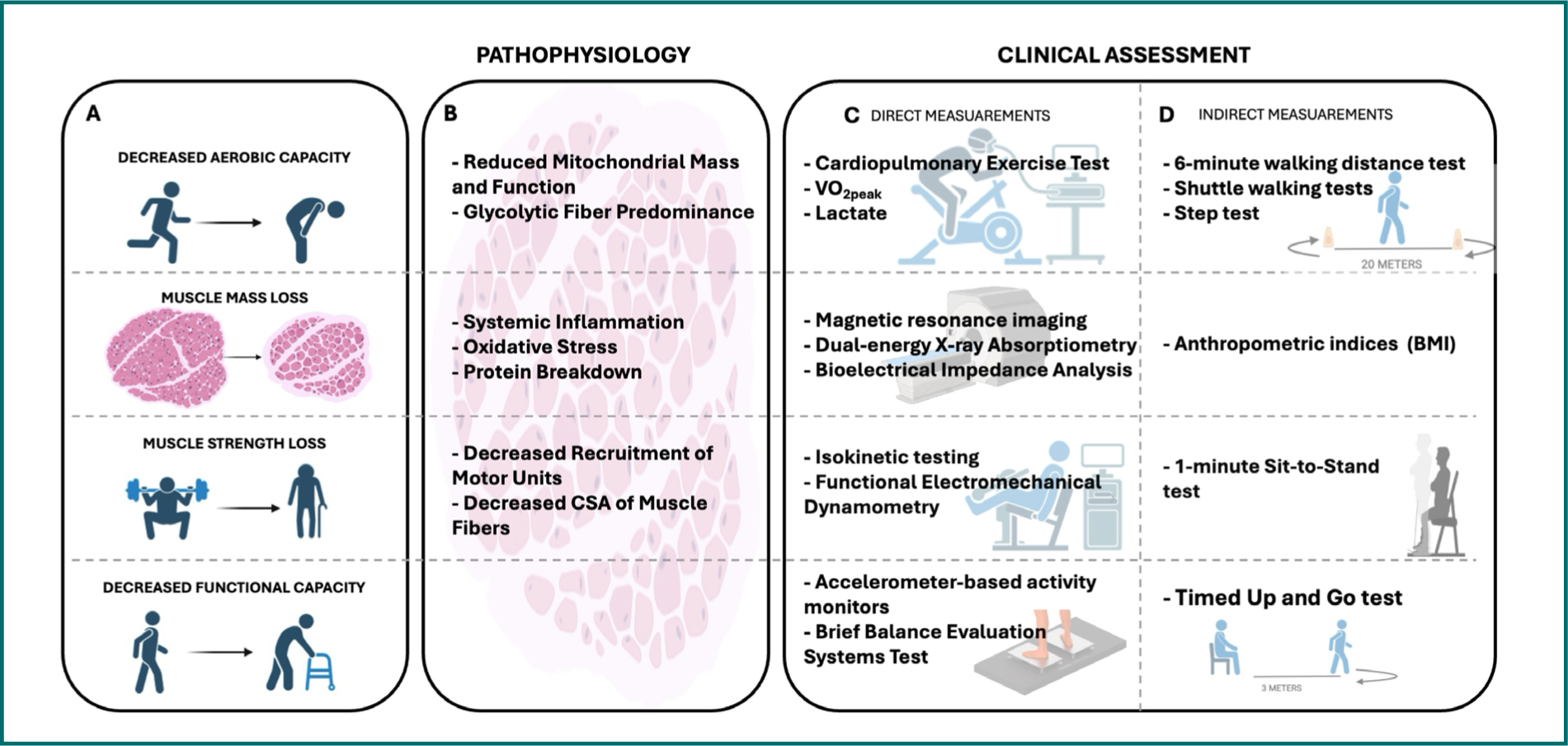
Figure 1. Pathophysiological mechanisms and clinical assessment of skeletal muscle dysfunction in COPD. A: clinical and functional manifestation of skeletal muscle dysfunction. B: underlying pathophysiological mechanisms within skeletal muscle. C: direct assessment tools used to characterize skeletal muscle impairment. D: indirect assessment tools used to evaluate the impact of skeletal muscle impairment.
These alterations should not be viewed in isolation but rather as interdependent processes that collectively contribute to SkM dysfunction in COPD. Disruptions in mitochondrial function, muscle composition, and contractile properties ultimately manifest as impairments in muscle endurance and strength, and body composition.11,17 Fortunately, these deficits can be captured through clinically accessible functional and morphological assessments (Fig. 1C and D). However, physiological and functional measurements may yield different interpretations depending on what is directly measured. For instance, maximal exercise capacity describes the body’s highest physiological or structural response to exercise (e.g., VO2max or maximal muscle contraction), whereas functional capacity reflects a patient’s maximum ability to perform standardized functional tasks (e.g., walking or standing from a chair), highlighting the importance of linking clinical measurements to their underlying physiological mechanisms.
Therefore, this mini-review aims to synthesize current evidence on the most relevant clinical factors and pathophysiological mechanisms underlying SkM dysfunction in COPD, with particular emphasis on how molecular and cellular alterations translate into mechanical and functional outcomes. A clearer understanding of these interconnected processes may help refine clinical interpretations.
Reduced aerobic capacity in patients with COPD
Skeletal oxidative capacity is closely related to the number of functional mitochondria in the tissue.21 Mitochondria play a central role in SkM bioenergetics and redox homeostasis, processes that are disrupted in COPD.22 Molecular analyses of vastus lateralis (VL) biopsies from patients with COPD reveal reduced expression of electron transport chain components and decreased citrate synthase activity.23 Together, these alterations indicate a loss of mitochondrial mass and function, a finding corroborated by electron microscopy, which reveals fewer mitochondria of smaller size.24 Furthermore, a consistent finding across studies is a shift in muscle fiber-type composition, characterized by an increased proportion of glycolytic fibers and reduced SkM oxidative capacity.25 At the functional level, these structural alterations are associated with impaired oxidative phosphorylation and reduced ATP availability. Clinically, these alterations may contribute to early-onset fatigue and exercise intolerance in patients with COPD (Fig. 1B).26
Cardiopulmonary exercise testing (i.e., CPET), including measurement of maximal oxygen uptake (i.e., VO2max), is considered the gold standard for assessing exercise capacity.27 The impaired exercise capacity of COPD patients as derived from symptom-limited incremental exercise protocols, such as the VO2peak, can be summarized as: (a) mechanical constraint on tidal volume expansion, (b) abnormalities in oxygen transport, and (c) gas-exchange abnormalities.28 The CPET is a non-invasive technique that provides an evaluation of the integrative function of pulmonary, cardiovascular, hematopoietic, neuropsychological, and metabolic systems during maximal exercise (or intense physical stress), which allows the assessment of physiological reserves of these systems that are not adequately reflected through the assessment of each individual organ system at resting conditions.29 The CPET provides integrative information on oxygen uptake, ventilation, delivery to peripheral tissues, and utilization by SkM mitochondria.30 Although VO2peak is not a specific measure of mitochondrial function, as it is derived from symptom-limited efforts, it is generally regarded as a reliable indicator of overall oxidative capacity24 and as a marker of other factors that may limit exercise capacity in patients with COPD (e.g., cardiac ischemia).31 However, if this test is accompanied by capillary lactate measurements during submaximal24 or maximal25 exercise, it may be more informative about SkM metabolism in COPD (Fig. 1C).
Physical performance test
Despite their diagnostic value, CPET and associated metabolic measurements may not be available in all clinical or research settings. Consequently, less expensive and easier to perform tests, such as the 6-min walking distance test (6MWT) and the shuttle walking tests – including incremental shuttle walking test (ISWT), and endurance shuttle walking test (ESWT) – can be used to evaluate the level of exercise tolerance (Fig. 1D).32 These tests provide clinically meaningful information on functional performance but do not allow precise identification of the physiological mechanisms underlying exercise limitation.33
The shuttle walking tests are simple, well-tolerated, and externally paced, with minimal learning effects, but they require time-consuming instructions and are less validated than the 6MWT.34 In the ISWT, walking speed is determined by acoustic signals, and distance is the main outcome. In contrast, in the ESWT, a constant signal is used to assess submaximal capacity, with exercise duration as the outcome. These two tests are considered more standardized than the 6MWT, as walking speed is set and thus less influenced by motivation, self-selected pacing, or variability in the instructions provided.32
The step test has also been proposed as a surrogate of the incremental peak oxygen consumption test.34,35 In this test, exercise tolerance and desaturation can also be assessed in a smaller space (1 m2 and a stair) than in the 6MWT,36 which requires a large (20-30 m) corridor.35 In addition, constant-workload tests at submaximal intensities assess exercise duration and provide insight into limiting symptoms. They use standardized protocols, allow measurement of multiple physiological variables, and offer practical advantages of treadmill and cycle ergometry. However, treadmill workload is influenced by body weight and pacing, unlike cycling.37 Nevertheless, indirect tests are influenced by multiple sources of variability, including anthropometric characteristics, patients’ motivation, comorbidities, learning effects, and day-to-day fluctuations in performance.38
Balance and daily physical activity in COPD
Balance impairment is increasingly recognized as a relevant functional limitation in COPD patients and can be evaluated directly using posturography or force plates (Fig. 1C), and indirectly using a range of static and dynamic clinical tests (Fig. 1D).39 Common static balance assessments include the tandem stance and unipodal stance test. In contrast, dynamic balance is frequently assessed using the timed up and go (TUG) test. Balance can also be assessed through functional performance tests such as the Berg Balance Scale (BBS) and the Brief Balance Evaluation Systems Test, which examine multiple aspects of balance control. These tools are efficient, well accepted by clinicians, and suitable for balance screening.40 The TUG is a reliable predictor of falls in COPD, with observed differences exceeding clinically important thresholds, likely influenced by muscle fatigue and increased respiratory demands. Similarly, lower BBS scores in COPD patients indicate significant impairment in functional balance beyond the minimum detectable change.41
Functional performance can also be assessed through direct observation of daily activities or validated questionnaires, including the pulmonary functional status and dyspnea questionnaire, the pulmonary functional status scale, the London chest activity of daily living, and the Canadian occupational performance measure.42 In addition, physical activity in daily life can be objectively quantified using motion-sensor technologies, including pedometers, wearable devices, and accelerometer-based activity monitors, which provide information on the duration, frequency, and intensity of habitual activity in both healthy individuals and those with COPD (Fig. 1C).43
Although functional tests correlate closely with direct measures of maximal aerobic capacity, improvements in one domain are not necessarily accompanied by measurable changes in the other. In this context, Abdellaoui et al. reported that 6 weeks of endurance training in patients with COPD led to improvements in muscle mitochondrial function, which were closely associated with increases in 6MWT performance, despite the absence of significant changes in VO2peak.44 Such discrepancies between direct assessment of maximal aerobic capacity (VO2peak) and functional performance tests (e.g., 6MWT, Shuttle test, and step test) may reflect improvements in other muscle aspects, such as muscle strength and mechanical and/or oxidative efficiency.44 It is possible that, due to improved muscle force transmission induced by stiffer muscle and extracellular matrix structures, such as tendons and fascia, better physical performance is achieved without increased oxygen consumption.45 In addition, training-induced changes in fatigue tolerance and perceptual responses to exertion may also contribute to enhanced exercise tolerance.46 However, the relative contribution of SkM adaptations compared with mechanical or perceptual factors remains poorly defined in COPD.
Taken together, functional and balance assessments provide clinically meaningful information on patients’ performance and disability, but they do not allow precise identification of the physiological mechanisms underlying exercise limitation. Moreover, interpretation of functional performance should consider the influence of coexisting conditions frequently present in COPD patients, such as aging-related sarcopenia, cardiovascular disease, and metabolic disorders.47–49 All three have been independently associated with reduced physical performance and may further aggravate functional impairment in patients with COPD, while their underlying mechanisms are only partially shared with those described in COPD-related muscle dysfunction.47,50 When such coexisting conditions are identified, a more individualized assessment and management strategy, including appropriate treatment of cardiometabolic conditions and nutritional support when indicated, may be required to effectively address functional decline. Therefore, the combined use of complementary assessment methods is recommended to more accurately characterize SkM oxidative capacity and functional impairment in patients with COPD.
Muscle wasting and body composition changes induced by COPD
Muscle wasting is a structural manifestation of SkM dysfunction in COPD and is influenced by several overlapping pathophysiological mechanisms (systemic inflammation, hypoxemia, and oxidative stress) as well as clinical factors (malnutrition, physical inactivity, and corticosteroid exposure).51–54 These factors are associated with increased protein breakdown and mitochondrial dysfunction (Fig. 1B), which together contribute to progressive loss of muscle mass and reduced contractile capacity.52,53 Early detection of muscle loss allows timely implementation of targeted interventions, including nutritional support and exercise-based pulmonary rehabilitation, which have been shown to improve muscle mass, strength, and quality of life in patients with COPD.51,54,55
Muscle wasting affects approximately 15-40% of patients with COPD and increases with disease severity.51–53,56 Loss of fat-free mass (FFM), particularly in the lower limbs, is often more pronounced than changes in body weight or body mass index, indicating that muscle loss may be substantially underestimated when body mass alone is measured (Fig. 1D).56–58 Segmental body composition analysis has shown that muscle mass loss primarily affects the lower limbs, whereas upper-limb muscle mass remains relatively preserved across disease stages.56,59 Given the limitations of anthropometric indices, accurate assessment of body composition using techniques such as magnetic resonance imaging (MRI), dual-energy X-ray absorptiometry, or bioelectrical impedance analysis is essential for identifying muscle wasting in this population.51,60,61 For instance, thigh MRI studies in patients with COPD consistently report a regional pattern of muscle atrophy, with greater loss of muscle mass in the mid and proximal regions of the knee extensor muscles (Fig. 1C).60 These findings are consistent with the functional vulnerability of locomotor muscles in COPD.
Contractile dysfunction, muscle power, and functional outcomes
The structural and metabolic alterations underlying muscle wasting translate into measurable impairments in muscle contractile function.62 Emerging but still limited evidence suggests that neuromuscular factors may contribute to impaired muscle performance. In this context, Gulbas et al. reported increased single-fiber electromyography jitter values in patients with COPD, indicating disturbed neuromuscular junction transmission and suggesting delayed or unstable nerve-muscle signal propagation at the motor endplate.63 Such alterations may impair effective muscle activation during exercise (Fig. 1B). Consistently, reduced electrical activity of the VL muscle has been observed in COPD patients across low-, medium-, and high-intensity cycling,64 potentially limiting effective force production during dynamic exercise. Interestingly, patients with severe COPD may preserve quadriceps force-generating capacity when physical activity levels and FFM are maintained, suggesting that maximal strength can be relatively preserved despite marked muscle atrophy.65
These neuromuscular and contractile alterations have clear clinical implications, including a reduction in maximal muscle strength and aerobic capacity, which are associated with poorer performance on functional clinical tests such as the 6MWT, which reflects functional capacity, and with reduced performance on the sit-to-stand test (risk of falling).66,67 Notably, accumulating evidence from clinical studies suggests that muscle power using repetitive actions such as the 1-min sit-to-stand test, rather than strength or endurance, may be a more sensitive determinant of performance (Fig. 1D).67,68 This likely reflects the time-constrained nature of these tasks, which require rapid generation of submaximal force, efficient neuromuscular coordination, and effective transmission of force to repeatedly overcome body mass during functional movements. However, functional performance could also be influenced by the learning effect of the task (neural strategies) and by cognitive impairments of the individuals, which vary among patients with COPD.69
Future perspective
SkM dysfunction in COPD remains a complex and multifactorial condition in which biological mechanisms and clinical factors interact. Future research should prioritize longitudinal studies that integrate molecular and histological analyses of SkM with physiological, functional, and imaging-based assessments to clarify the relative contributions of mitochondrial dysfunction, neuromuscular alterations, systemic inflammation, and deconditioning to exercise intolerance.70 Clarifying the relative contribution of SkM adaptations compared with mechanical or perceptual factors remains an important research priority. Moreover, the role of inactivity as a cause or an aggravating factor needs further exploration. Future investigations are needed to determine how different rehabilitation strategies influence specific muscle phenotypes and whether targeted interventions can be tailored to individual muscle characteristics.71
Conclusion
Available literature shows that COPD is a systemic and multifactorial disease in which SkM dysfunction, particularly affecting the lower limbs, plays a central role in exercise intolerance, functional limitation, and adverse clinical outcomes. Alterations in muscle composition, mitochondrial structure and function, and body composition converge to reduce oxidative capacity, adenosine triphosphate availability, and force-generating capacity, thereby promoting early fatigue, a consistent finding across clinical and experimental studies.
Muscle wasting, together with declines in muscle strength and power, is closely associated with poorer performance in clinically relevant functional tests such as the 6-min walk and sit-to-stand tests, underscoring the impact of SkM dysfunction on daily activities and prognosis. Importantly, no single clinical test fully captures the complexity of muscle impairments in COPD. However, among currently available field-based assessments, the 1-min sit-to-stand appears particularly sensitive to lower-limb muscle dysfunction because of its reliance on repeated rapid force generation. In contrast, the 6-min walk test provides complementary prognostic information by reflecting whole-body functional capacity.
Taken together, these observations highlight the importance of comprehensive and multimodal assessment of muscle health in patients with COPD, integrating measures of muscle mass, functional performance, and exercise capacity. Such an approach is essential for guiding early, targeted interventions combining nutritional strategies and exercise-based pulmonary rehabilitation, with the ultimate goal of improving functional capacity and quality of life.
Funding
This project was funded by FONDECYT #1260589 (LP), ANID POST-DOCTORADO # 3240206 (CC), and Nucleo UNAB # DI-03-23/NUC (LP).
Conflicts of interest
None.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from all patients, and secured approval from the Ethics Committee. SAGER guidelines have been followed as applicable to the nature of the study.
Declaration on the use of artificial intelligence. The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
