Introduction
Muscle dysfunction in chronic respiratory diseases (CRDs) encompasses loss of maximal force and/or premature fatigability in respiratory and/or limb muscles. It is highly prevalent in chronic obstructive pulmonary disease (COPD) and occurs across other CRDs, often independently of airflow obstruction or restriction severity and traditional physiological metrics.1–21 Beyond symptoms, muscle dysfunction impairs daily activities, worsens quality of life, delays recovery after exacerbations, and portends poorer survival.3,8,11,21–25 A clinically grounded synthesis is needed for practitioners to recognize dominant drivers in each condition and to link them to actionable interventions. Here we (I) present a conceptual framework for clinical causes of muscle dysfunction; (II) detail diseasespecific patterns with emphasis on COPD; (III) summarize practical assessment; and (IV) outline therapeutic implications with preset bestevidence recommendations.
Conceptual framework: domains and interactions
Most of the clinical causes of muscle dysfunction can be grouped into eight partially overlapping domains that differentially affect respiratory and limb muscles (Fig. 1).
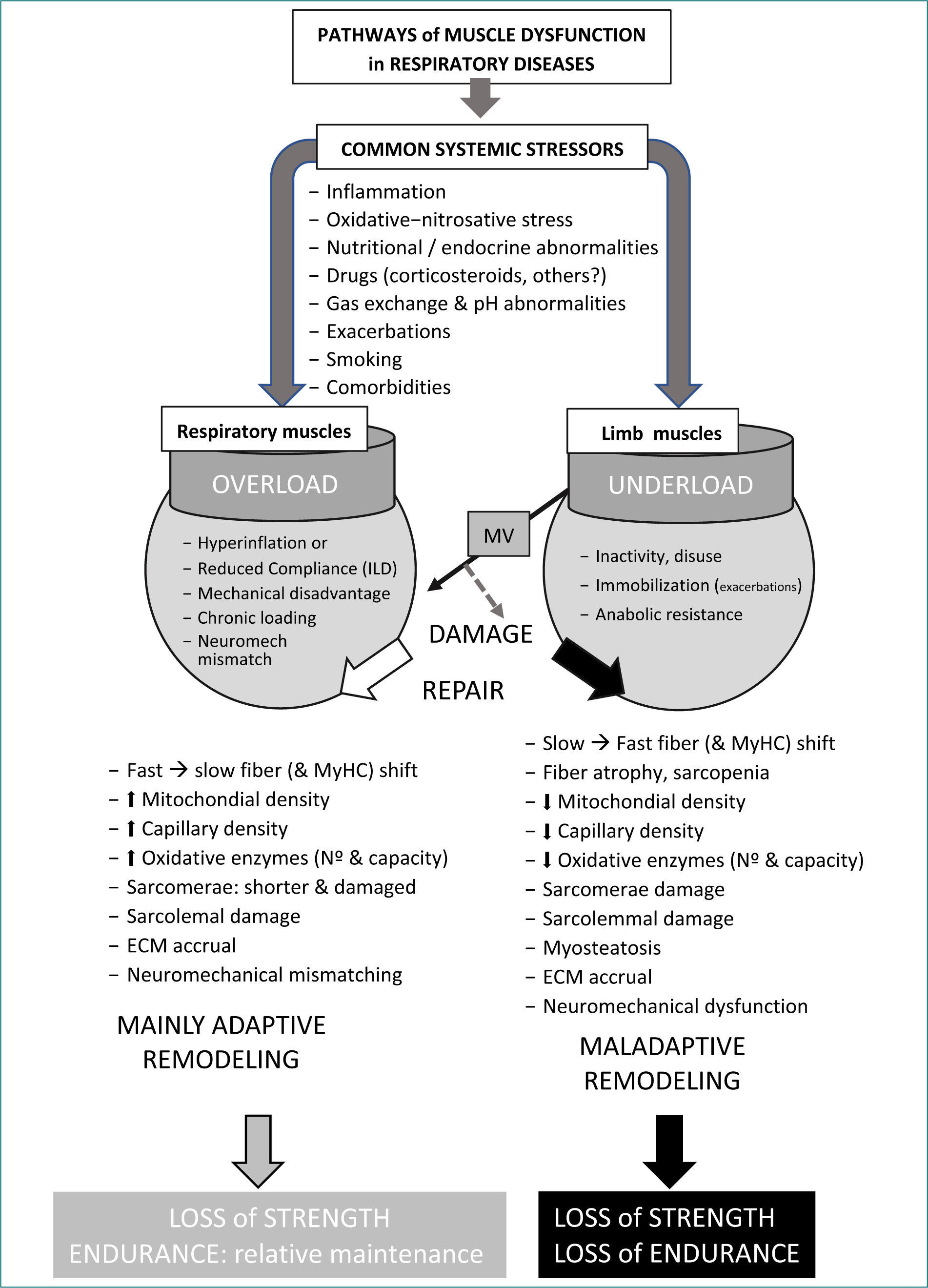
Figure 1. Factors, mechanisms and functional consequences of muscle dysfunction in COPD and other chronic respiratory diseases
Ventilatory loads and geometry of respiratory muscles
Both static and dynamic hyperinflation shorten the diaphragm and flatten its dome,26,27 whereas the opposite effect is applied to intercostals and parasternals.27,28 These changes reduce the pressure-generating capacity of respiratory muscles;26 generating low thoracic compliance and increasing airway resistance, thus resulting in the augment of work of breathing and increased dyspnea. The resulting limitation indirectly affects limb muscles through the resulting deconditioning.
Physical inactivity and deconditioning
Reduced daily activity secondary to airflow limitation promotes limb muscle atrophy and oxidative deconditioning,11 with smaller fibers, a higher proportion of type II fibers, reduced capillarity, and diminished mitochondrial density and oxidative capacity.29–31 These adaptations appear to be greater in the lower than in the upper limbs, probably reflecting preferential disuse of the legs compared with the arms.32,33
Muscle systemic environment
Chronic inflammation, oxidative stress, and gas exchange abnormalities promote proteolysis, impair excitation-contraction coupling, and reduce endurance in all muscle groups.34–37
Nutritional state and anabolic-catabolic balance
Inadequate protein intake and a predominant systemic catabolism, affecting mostly proteins and lipids, underpin the sarcopenic phenotype in many respiratory patients.11,38
Iatrogenic factors
Tobacco, as well as treatments with systemic corticosteroids and other drugs, may contribute to muscle dysfunction in susceptible patients.39–41
Comorbidities and aging
Coexistence of different CRDs and other chronic conditions, such as cardiovascular and renal diseases, diabetes, and osteopenia, as well as aging, all of which are frequent in respiratory patients, can further contribute to muscle dysfunction. Notably, many of these latter conditions share pathogenic mechanisms with CRDs, including physical inactivity, systemic inflammation, oxidative stress, and anabolic resistance.11,42–44
Exacerbations
Acute inflammatory/metabolic stressors, more pronounced inactivity, and frequent steroid bursts used in these acute events create cumulative, stepwise losses in muscle structure and function.45–47
Damage and differences in regenerative capacity
Variability in satellite cell pool/function and hormonal milieu may modulate recovery and adaptation of muscles in CRDs.45,48–52
Interaction between systemic drivers and disease-specific mechanical loads
Although the above domains are described separately for conceptual clarity, in clinical practice, muscle dysfunction results from the interaction between systemic biological drivers and disease-specific mechanical loads imposed by the respiratory system. In COPD, for instance, static and dynamic hyperinflation place inspiratory muscles at a shortened operating length and increase inspiratory loading. When this mechanical disadvantage occurs in the context of systemic inflammation, oxidative stress, hypoxemia, nutritional depletion, and/or anabolic resistance, the capacity of both respiratory and limb muscles to adapt may be compromised. Conversely, in restrictive disorders, such as interstitial lung diseases (ILDs), the dominant mechanical constraint is increased elastic loading due to reduced lung compliance, which interacts with similar systemic modifiers to determine the final muscle phenotype and function. In other words, skeletal muscle dysfunction in CRDs emerges from the convergence of respiratory mechanical constraints and systemic metabolic–inflammatory environments, with different weighting across diseases.
Clinical assessment essentials
Because skeletal muscle impairment materially affects prognosis and treatment responsiveness, routine CRDs evaluation should include targeted functional and nutritional phenotyping.
Semiology
Orthopnea or exertional tachypnea, paradoxical breathing, weak cough, and/or limb fatigability suggest muscle dysfunction.
Functional assessment for respiratory muscles
Respiratory pressures can be screened using mouth (maximal inspiratory pressure [MIP]/maximal expiratrory presure [MEP]) or sniff nasal inspiratory pressure (SNIP) determinations (SNIP), with more mechanistic testing (e.g., determination of transdiaphragmatic pressure [Pdi] or twitch techniques) reserved for specialist settings.10,53,54
Functional assessment for limb muscles
Although handgrip (HG) dynamometry provides a rapid global marker of peripheral muscle function, lower-limb assessment (e.g., quadriceps force) is often more-disease relevant.11,23,55
Nutritional assessment
Calculation of body mass index (BMI), or preferably, variables reflecting body composition, is also essential for evaluating nutritional status. Although BMI is the simplest metric, it cannot detect sarcopenic obesity (i.e., preserved body weight with reduced muscle mass), which is relatively common in patients with CRDs. Accordingly, lean-mass-normalized indices (e.g., fat-free mass index [FFMI] determined by electrical bioimpedance or dual-energy X-ray absorptiometry [DXA]) are preferred to detect clinically relevant muscle depletion in overweight/obese CRDs presentations.11,56,57 This can be complemented by determinations of laboratory parameters.
Activity profiling
The use of specific questionnaires, accelerometers, and step counts capture the physical inactivity-deconditioning loop, and can monitor response to interventions in this dimension. Its thresholds and interpretive nuances are detailed in respiratory society guides and pragmatic clinical reviews.58–61 Importantly, exercise capacity and physical activity are not equivalent concepts. The former assesses physiological potential (the “capacity”), whereas the latter is influenced not only by this but also by motivation and context of execution. Therefore, measures aimed at increasing physical activity in patients with CRDs should address both dimensions simultaneously.
In the following paragraphs, the particular circumstances that contribute to muscle dysfunction across different CRDs are examined.
COPD: clinical drivers, patterns, and consequences
Limb muscles: inactivity and deconditioning
Reduced physical activity is a hallmark of COPD, present even in early stages. Limb muscle deconditioning follows,11 being characterized by whole muscle and fiber atrophy and a shift from oxidative toward glycolytic metabolism, with increased percentage of type II fibers, reduced capillarity, and mitochondrial dysfunction.29–31 Clinically, this translates into lower quadriceps strength, reduced endurance, and earlier lactate accumulation during constantwork exercise. Inactivity is amplified by dyspnea, fear of exertion, exacerbations, and comorbidities.11,45,62,63 Importantly, limb weakness independently predicts exercise intolerance, readmissions, and mortality after adjusting for FEV1 and respiratory gas exchange.23,64,65
Respiratory muscles: hyperinflation and mechanical disadvantage
Chronic air trapping (static hyperinflation) and episodic volume expansion during exertion or acute worsening (dynamic hyperinflation) displace the diaphragm to a shorter operating length and reduce its appositional contact with the rib cage, thereby lowering pressure output.26,27 In parallel, thoracic configuration changes modify the length-tension conditions of intercostal and parasternal muscles.27,28 Superimposed intrinsic end-expiratory pressure increases the inspiratory “opening” load, further elevating the mechanical burden at the start of each breath. Sustained ventilatory loading can promote oxidative and fatigue-resistant remodeling in inspiratory muscles (“training effect”).66,67 However, these adaptations are typically insufficient to normalize peak force-generating capacity because the underlying geometric disadvantage persists.26 The clinical consequence is a phenotype in which endurance may be relatively preserved compared with maximal strength, contributing to symptoms and inefficient ventilatory patterns under stress. Interventions that reduce end-expiratory lung volume can partially restore inspiratory muscle mechanics and improve exercise tolerance. This includes pharmacologic deflation with bronchodilators, ventilatory approaches that mitigate dynamic hyperinflation, and (in appropriate emphysema phenotypes) surgical or endoscopic lung-volume reduction techniques.68–71 When indicated, adjunct respiratory muscle training may further enhance functional performance.72,73
Systemic additional contributors
INFLAMMATION AND OXIDATIVE STRESS
These phenomena are linked to proteasome activation and impaired contractility. Exacerbations (see below) intensify these insults.45,74,75
GAS EXCHANGE ABNORMALITIES
Hypoxemia, with or without hypercapnia and acidosis, reduces muscle endurance and impairs mitochondrial function.76–78 Oxygen therapy and ventilatory support can mitigate these effects.
NUTRITIONAL ABNORMALITIES
Weight loss leading to low BMI and FFMI is frequent.11,57 Notably, the cachexia phenotype portends worse outcomes.56
HORMONAL/ANABOLIC DEFICITS
Relative anabolic resistance and hypogonadism have been documented in subsets of COPD patients.79–81
MEDICATIONS
Systemic corticosteroids, particularly with long-term use, can contribute to myopathy;40,41 in susceptible patients, other drugs may also predispose to myopathy or tendinopathy.82,83
ADDITIONAL ABNORMALITIES WITHIN THE MUSCLES
Intermuscular adiposity is common and has been associated with reduced oxidative capacity and strength.84,85 Furthermore, impaired regenerative capacity (reduced satellite-cell number or function) has been reported in sarcopenic COPD.45,48
Exacerbations as accelerators
Exacerbations act as “catabolic shocks” that combine abrupt activity restriction with systemic inflammatory activation, worsened gas exchange, transient surges of dynamic hyperinflation, and repeated exposure to systemic glucocorticoids.41,46,47 Recurrent events, therefore, generate a cumulative trajectory of functional loss, with declines in limb strength and endurance, and potential deterioration in respiratory muscle performance.86,87 This supports early mobilization and rapid post-event rehabilitation as core components of care in frequent-exacerbator phenotypes.88,89
Prognostic impact
Quadriceps weakness, low FFMI, and reduced activity independently predict hospitalizations and mortality.23,56,90 Respiratory muscle weakness adds risk for ventilatory failure, difficult weaning, and postoperative complications, and has also been reported as an independent predictor of mortality.91–93 Integrating muscle assessments into routine COPD evaluation refines risk stratification beyond spirometry alone.
Muscle dysfunction has been predominantly studied in COPD. However, many of the elements discussed in the preceding section also apply to other CRDs. Accordingly, the next parts will address only the most distinctive features of these other conditions, without repeating material already covered.
Asthma
Bronchial asthma typically presents with reversible airflow limitation, but airway remodeling can lead to chronic obstruction in some patients. Baseline limb and respiratory muscle function is often preserved in wellcontrolled asthma. However, two clinical drivers stand out in this CRD. First of all, systemic corticosteroid exposure,16 which is associated with proximal limb weakness and, in severe cases, acute myopathy. Weakness often reflects type II fiber atrophy94 and typically improves with tapering, though recovery may be protracted. Second, episodic hyperinflation and hypoxemia during severe attacks transiently degrade inspiratory muscle mechanics by increasing the work of breathing. However, even in chronic asthma, respiratory muscle function is roughly preserved or only moderately impaired.14,95–97 It is possible that this reflects adaptive mechanisms similar to those observed in COPD. In fact, diaphragm thickness appears to be slightly increased.95 However, robust structural or metabolic data on the respiratory muscles of asthma patients are lacking. In cases of severe asthma exacerbations, rhabdomyolysis has been documented, although the muscle source of the enzymatic biomarkers remains unclear.98,99 Physical inactivity may emerge in poorly controlled asthma due to fear of symptoms, contributing to deconditioning. It is worth noting that adults with asthma show lower habitual activity than healthy controls.100,101 Structural and metabolic data are slightly more abundant for limb muscles in patients with asthma. Evidence of oxidative stress and mitochondrial dysfunction has been reported,102 along with low magnesium content, a finding that may suggest sarcolemmal instability.103 Steroidsparing strategies, graded exercise training, selective inspiratory muscle training in deconditioned or hyperinflationprone patients, and optimal asthma control will improve symptoms and functional outcomes in stable patients.
ILD
ILD are a heterogeneous group of parenchymal disorders marked by inflammation and fibrosis that involve not only pulmonary but also exerted multisystemic effects, including those involving skeletal muscles.104–106 ILDs impose a high, chronic ventilatory load because of a restrictive pattern and reduced lung compliance, and often associate exertional hypoxemia.104 Patients commonly exhibit dyspnea, especially when exercising, reduced physical activity, and weight loss. Limb muscle weakness and endurance impairment predominate;7,106,107 whereas inspiratory muscles face sustained loads. However, the diaphragm becomes less affected than in other CRDs.7,43 Nutritional abnormalities, systemic inflammation, steroid and/or antifibrotic drug exposure in subgroups of patients, and comorbidities further contribute to muscle dysfunction.7,43,108–110 Pulmonary rehabilitation improves functional outcomes;111–114 and supplemental oxygen during training attenuates hypoxemic limitations. Nutritional assessment is essential, and anabolic strategies may be considered casebycase.
Cystic fibrosis (CF) and non-CF bronchiectasis
Chronic infectiondriven inflammation, recurrent exacerbations, and increased work of breathing shape muscle dysfunction in advanced bronchiectasis.20,115–117 This is associated with significant nutritional problems both in CF patients with uncontrolled pancreatic insufficiency and in some subgroups with non-CF bronchiectasis (particularly evident in women).20,118 Limb muscle weakness and reduced endurance are common in CF and non-CF bronchiectasis;5,20 and expiratory muscles may be strained by chronic cough, yet usually maintain strength at rest in less severe diseases. Addressing infection control, nutrition (particularly in CF), and structured training are central in the management of these two groups of patients.119,120
Sleep apnea syndrome (SAS)
SAS and related disorders are characterized by recurrent episodes of complete or partial upper-airway collapse during sleep. These events lead to nocturnal hypoxemia, disruption of sleep architecture, and daytime hypersomnolence.121 Skeletal muscle dysfunction has also been reported in these sleep disorders, particularly in patients with obstructive SAS. In this setting, reductions in strength and endurance may be observed in both respiratory and limb muscles, whereas increased fatigability seems to be confined mainly to the former.1,4 These alterations have been linked to the lack of restorative sleep and, above all, to intermittent hypoxia-normoxia cycles.122,123 However, inspiratory muscles repeatedly generate progressively submaximal efforts during apneic events,124 which could promote fatigue yet also resemble a training stimulus. Accordingly, inspiratory muscle strength and endurance appear to be broadly preserved in many patients with SAS.1,4,125 Nevertheless, their safety margin against fatigue is reduced,1 particularly in severe disease. In parallel, functional deficits are accompanied by cellular and molecular changes. The external intercostal, for instance, has shown larger type II fibers together with reduced oxidative stress and a lower proportion of aerobic fibers.126 Limb muscles, in turn, have elicited a higher number of blood-vessels.127 This enhanced capillarity is likely driven by VEGF overexpression in response to repeated hypoxic bouts.128 Although continuous positive airway pressure (CPAP) improves sleep quality and decreases nocturnal ventilatory load, it only partly restores respiratory muscle performance.1,126 This incomplete recovery may relate to persistent muscle oxidative stress126 and possibly to pulmonary hyperinflation induced by CPAP. Finally, upper-airway muscles, which are key contributors to SAS pathophysiology, also exhibit mechanical and metabolic adaptations.129–131
Chest wall disorders and neuromuscular diseases
Kyphoscoliosis, scoliosis, and other chest wall disorders confer a mechanical disadvantage on the respiratory muscles and reduce chest wall compliance.12,19 Chronic hypoventilation and nocturnal hypoxemia, with or without hypercapnia, are frequent in these patients, who typically reduce their physical activity secondarily and develop limb muscle deconditioning.19 Primary neuromuscular diseases, in turn, involve intrinsic muscle or motor-unit pathology, with secondary deconditioning and nutritional issues.122 Some of these disorders also involve muscle damage and subsequent fibrosis.122 Therapeutic measures for muscle dysfunction in these populations involve non-invasive ventilation, with transition to invasive ventilation in selected cases; cough augmentation (sometimes using assistive technologies); and targeted physiotherapy, with exercise applied judiciously according to diseasespecific guidelines.132,133
Measurement pearls for clinicians
– FFMI is more informative than BMI for detecting sarcopenia/cachexia and should be included in the evaluation of CRDs patients.
– The level of physical activity, assessed by questionnaires or wearable devices, is important to identify individuals at risk of deconditioning and muscle dysfunction.
– Image techniques (e.g., computed tomography, ultrasonography, and MRI) enable assessment of the phenotype (structure and mass) and even function of specific muscle groups. New markers, such as the myoesteatosis index or the diaphragmatic thickness have come to the fore given their prognostic implications.
– Maximal pressures (MIP/MEP or SNIP) are clinical tests useful for assessing respiratory muscle strength, whereas handgrip and quadriceps dynamometry are appropriate options to evaluate limb muscle strength.
– Muscle function should be reassessed after exacerbations, because these acute events worsen performance.
– Beware rapid proximal weakness during highdose or prolonged systemic corticosteroid therapy.
Therapeutic implications across CRDs
Clinical management implications
A range of measures can be implemented to offset, at least partially, the effects of muscle dysfunction in CRDs:
PULMONARY REHABILITATION
It is recommended to combine highintensity endurance training (at least 3 sessions/week) with progressive resistance exercises (2-3 sets of around 10 repetitions) for limb muscles. These exercises should be individualized to deliver the load required to achieve the objective, while at the same time taking into account the symptomlimited thresholds. In severely limited patients, for instance, training intensity should initially be tailored to symptom-limited thresholds, typically corresponding to moderate intensity (e.g., 50-60% of peak work rate or equivalent perceived exertion), with gradual progression as tolerance improves. Interval training strategies may be particularly useful in patients with marked ventilatory limitation or dynamic hyperinflation. Telerehabilitation and home-based programs are also very promising tools.
INSPIRATORY MUSCLE TRAINING
It is also important to consider adding thresholdloaded inspiratory training in patients with demonstrable weakness or high ventilatory loads. This can improve their exercise performance. Present evidence supports threshold-loaded inspiratory muscle training at loads of approximately 30-50% of MIP, performed in daily or at least 5 days/week sessions of 20-30 min,72 with periodic adjustment of the load as strength improves.
DEFLATION STRATEGIES
Bronchodilators are the simplest way to achieve this objective. In selected patients with emphysemapredominant phenotypes, consider surgical or endoscopic lung volume reduction.
OXYGENATION AND MECHANICAL VENTILATION
Correct hypoxemia and consider nocturnal or ambulatory non-invasive ventilatory support when indicated. In patients with exertional hypoxemia (particularly in ILD and advanced bronchiectasis), supplemental oxygen during exercise training can improve tolerance and allow higher training intensity. In these cases, oxygen flow should be titrated to maintain adequate oxygen saturation (commonly ≥ 88-90%) during exercise sessions.
NUTRITIONAL SUPPORT
Target appropriate energy/protein intake, and use oral nutritional supplements when needed. Remember that the effects of nutritional support will be enhanced if accompanied by an appropriate training program.
MEDICATION STEWARDSHIP
It is also important to minimize cumulative systemic steroid exposure and to carefully review other potentially myotoxic drugs. Consider Vitamin D supplementation and treat hypogonadism when appropriate.
EXACERBATION PREVENTION
Appropriate vaccinations, optimal inhaled therapy, intermittent antibiotic therapy in selected cases, selfmanagement plans, early rehabilitation, and activity coaching can help prevent exacerbations.
COMORBIDITY MANAGEMENT
Other chronic diseases and aging frequently coexist with COPD. Optimizing cardiovascular fitness, diabetes control, and osteoporosis prevention,
Conclusion
In COPD, locomotor muscle impairment is largely shaped by chronic underuse with downstream atrophy and metabolic remodeling, whereas inspiratory muscle dysfunction in primarily driven by hyperinflationinduced geometric disadvantage and increased inspiratory loading. Across both muscle compartments, systemic modifiers, such as hypoxemia, hypercapnia, acidosis, inflammation-oxidative stress, nutritional-endocrine disturbances, medication exposure (notably systemic corticosteroids), and exacerbation burden, interact to determine severity, recovery potential, and clinical impact. Similar mechanisms operate across other CRDs, but with disease-specific weighting (e.g., restrictive loading and exertional increased hypoxemia in ILD, steroid exposure and episodic hyperinflation in asthma, infection-driven systemic inflammation and malnutrition in bronchiectasis. Recognizing the dominant clinical drivers in each patient supports rational combinations of rehabilitation and targeted training, lung deflation and ventilatory strategies when indicated, optimization of oxygenation, and nutritional/metabolic support. Routine incorporation of muscle assessment can refine risk stratification and guide pragmatic, highvalue care.
Funding
Funded by PI25/01093 (ISCiii), co-funded by the European Union.
Conflicts of interest
J. Gea is a recipient of the Predoctoral Grant PFIS FI22/00003, ISCiii co-funded by the European Union.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. This study does not involve personal patient data, medical records, or biological samples, and does not require ethical approval. SAGER guidelines do not apply.
Declaration on the use of artificial intelligence. The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
